Improving hearing health workflow: a 2026 guide
- 6 days ago
- 8 min read

TL;DR:
A structured hearing health workflow, incorporating standardized protocols, digital tools, and evidence-based follow-up, improves patient outcomes and operational efficiency. Integrating hybrid teleaudiology and self-directed rehabilitation into decision-guided pathways enhances access, adherence, and scalability while reducing clinical variability. Effective care depends on unified documentation, proactive scheduling, and rigorous triage protocols to ensure safe, consistent, and high-quality audiology services.
A well-structured hearing health workflow, known in audiology practice as a clinical care pathway, is the single most reliable predictor of consistent patient outcomes and operational efficiency in hearing services. Improving hearing health workflow means applying standardised clinical protocols, adopting hybrid teleaudiology models, and integrating digital tools such as AI-supported documentation to reduce variability across every stage of care. The 2026 NICE guidelines for adult hearing loss have reinforced the importance of structured follow-up schedules, making this an opportune moment for audiology teams and ear care practitioners to reassess how their pathways are designed and delivered. This guide sets out the evidence-based strategies that make the greatest difference.
What are the essential clinical workflow steps for hearing health optimisation?
Effective hearing healthcare workflow optimisation begins with a clearly sequenced care pathway. Each stage must be purposeful, documented, and linked to the next so that no patient falls through the gaps between assessment and rehabilitation.
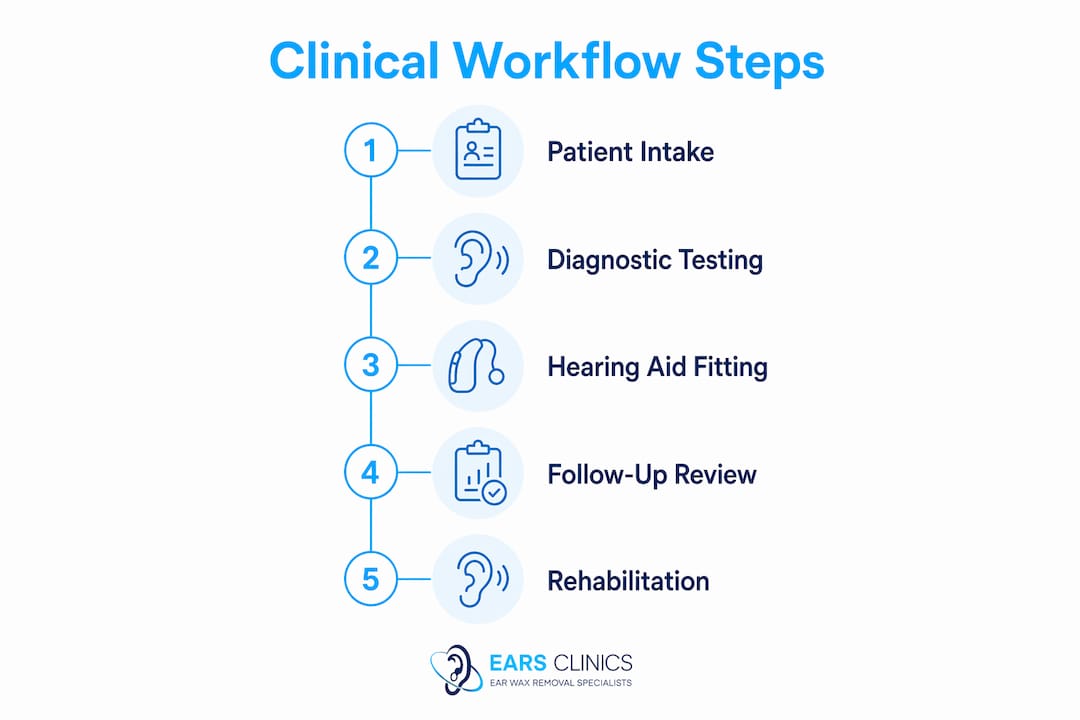
The core stages of a well-designed auditory care process are:
Earwax assessment and removal — Cerumen (earwax) impaction must be addressed before any audiological assessment. Microsuction is the method recommended by current NICE guidelines and is the preferred approach at EARS Clinics, though irrigation and manual instrumentation remain clinically valid options. Practitioners select the most appropriate technique based on the patient’s medical history and clinical presentation.
Audiological assessment — Pure tone audiometry, speech recognition testing, and tympanometry form the diagnostic foundation. Accurate baseline data at this stage determines every subsequent clinical decision.
Hearing aid fitting and counselling — Device selection, fitting, and patient education should be documented against personalised care goals, not generic outcomes.
Structured follow-up — NICE 2026 guidance recommends a face-to-face audiology follow-up 6 to 12 weeks after hearing aid fitting. This means follow-up timing is now a clinical standard, not a discretionary choice.
At the 6 to 12 week follow-up, clinicians should systematically review:
Hearing aid comfort and physical fit
Sound quality, volume settings, microphone performance, and noise reduction
Cleaning technique and battery management
Telephone use and compatibility with assistive listening devices
Device usage hours logged by the hearing aid data-logging function
Follow-up timing aligned with these actionable clinical checks ensures that workflows directly improve patient outcomes rather than simply filling appointment slots. Documenting personalised care goals at the fitting stage gives the follow-up consultation a clear reference point, reducing consultation drift and improving the quality of clinical decisions.
Pro Tip: Create a standardised follow-up checklist embedded directly in your clinical software so that every practitioner covers the same NICE-aligned review points, regardless of which clinician conducts the appointment.
How can digital tools and AI enhance hearing care workflows?
Digital tools are now central to hearing healthcare workflow optimisation, particularly in reducing the administrative burden that erodes clinical time. Audiology software platforms such as Auditdata have introduced AI Notes features that automatically transcribe counselling sessions and generate structured documentation outputs, including consultation summaries and patient letters. This matters because documentation inconsistency is one of the most common sources of clinical variability in multi-practitioner settings.
The practical benefits of embedding guided clinical workflows in audiology software include:
Enforced consistency — Mandatory data capture fields prevent incomplete records and support clinical governance requirements.
Reduced administrative time — Automatic transcription and structured output reduce post-consultation documentation from minutes to seconds.
Improved handoffs — Structured records make it straightforward for any clinician to pick up a patient’s care without losing context.
Scalability — Standardised workflows can be replicated across multiple clinic sites without quality degradation.
Standardising mandatory data capture within workflow systems addresses the root cause of clinical variability, which is inconsistent documentation and handoffs rather than individual practitioner competence. This is a critical distinction. Treating documentation, billing, and clinical decision points as one integrated system rather than three separate administrative tasks is what makes workflow improvements scalable across a growing practice.
Pro Tip: Before selecting audiology software, map your current documentation touchpoints and identify where data is duplicated or lost. Software that mirrors your existing clinical logic will be adopted faster and with fewer errors.

What are the best practices for hybrid and remote hearing rehabilitation workflows?
Hybrid teleaudiology models represent one of the most significant advances in enhancing the auditory care process for patients with access barriers. A hybrid teleaudiology model combines structured remote content delivery with synchronous counselling and early adherence assessment, and evidence from a northern India feasibility study demonstrates that this approach improves both accessibility and patient adherence. The model uses asynchronous multimedia rehabilitation videos alongside targeted motivational interviewing at follow-up, with adherence assessed at one month.
The table below outlines when remote follow-up is appropriate versus when an in-person visit is clinically necessary:
Clinical scenario | Recommended pathway |
Routine hearing aid adjustment, no reported pain | Remote synchronous appointment |
New hearing aid user, first follow-up | In-person (NICE 2026 standard) |
Cochlear implant programming, stable adult patient | Remote synchronous or asynchronous |
Cochlear implant, paediatric or new implant user | In-person with caregiver present |
Patient-reported sudden change in hearing | In-person triage, same session |
Adherence monitoring at one month post-fitting | Remote asynchronous or telephone |
Remote cochlear implant programming is clinically equivalent to in-person programming, with high satisfaction reported by both patients and professionals. This means that for stable adult cochlear implant users, remote follow-up is not a compromise but a clinically validated option that also reduces travel burden significantly.
Implementing a hybrid pathway effectively requires the following steps:
Define triage criteria at the point of discharge from initial fitting, specifying which future contacts will be remote and which require attendance.
Provide patients with asynchronous rehabilitation materials, such as instructional videos on device use and communication strategies, before their first remote follow-up.
Use patient-reported outcome measures (PROMs) and aided hearing evaluations to determine whether a remote check is sufficient or whether escalation to in-person care is required.
Schedule early adherence checks at four weeks to identify patients at risk of disengaging before problems become entrenched.
Remote care pathways should not default to fully remote delivery but be decision-guided to preserve quality and escalate in-person care when clinical flags arise. This principle protects both patient safety and clinical standards.
How to implement self-directed auditory rehabilitation alongside clinician-led care
Self-directed auditory rehabilitation is defined as structured training in speech and sound recognition that patients complete independently, using computer-based programmes, mobile applications, or instructional video content, outside of scheduled clinical appointments. It addresses two specific workflow bottlenecks: access to care and long-term adherence, without replacing the clinician’s role in assessment and fitting.
The evidence base is now substantial. Digital training programmes delivered at home for 20 or more hours show meaningful, sustained speech recognition improvements maintained up to three months post-training, across diverse adult populations. This means that self-directed rehabilitation is not a supplementary nicety but a clinically effective component of a complete hearing care pathway.
For practitioners designing or recommending self-directed programmes, the key considerations are:
Patient profile matching — Patients with mild to moderate hearing loss and good digital literacy are the strongest candidates for app-based or computer-based programmes. Those with more complex needs or lower confidence with technology benefit from instructional video formats with telephone support.
Session duration and frequency — Evidence supports sessions of 20 to 30 minutes, three to five times per week, as the threshold for producing durable gains. Shorter, irregular engagement does not produce the same outcomes.
Engagement strategies — Progress tracking, automated reminders, and brief clinician check-ins at four and eight weeks significantly reduce drop-off rates.
Operational integration — Clinics can extend their rehabilitation reach without proportional resource investment by prescribing self-directed programmes at the point of fitting and monitoring progress remotely.
Pro Tip: Prescribe self-directed auditory rehabilitation as a formal part of the care plan at the hearing aid fitting appointment, not as an afterthought. Framing it as a clinical recommendation rather than an optional extra increases patient uptake and adherence.
Combining self-directed rehabilitation with the structured follow-up schedule recommended by NICE 2026 creates a care pathway that supports patients between appointments, reduces the burden on clinic capacity, and produces better long-term hearing outcomes than clinician-led care alone.
Key takeaways
Improving hearing health workflow requires integrating structured clinical protocols, AI-supported documentation, hybrid teleaudiology, and self-directed rehabilitation into a single, decision-guided care pathway.
Point | Details |
Follow NICE 2026 follow-up standards | Schedule face-to-face review 6 to 12 weeks post-fitting, covering comfort, settings, and usage data. |
Integrate documentation as a clinical system | Treat documentation, billing, and clinical decisions as one unified process to reduce variability. |
Apply hybrid teleaudiology selectively | Use triage criteria to determine remote versus in-person care rather than defaulting to either. |
Prescribe self-directed rehabilitation formally | Recommend home-based auditory training programmes at fitting to extend care reach and improve adherence. |
Use graduated scheduling reminders | Send proactive reminders at 90, 60, and 30 days before key milestones to reduce reactive demand. |
What we have learned from building better hearing care pathways
The most persistent mistake we see in audiology workflow redesign is treating each stage of care as a separate process. Documentation sits with administration, clinical decisions sit with the audiologist, and billing sits with the practice manager. When these three functions are siloed, variability is inevitable and scalability becomes almost impossible.
The practices that improve most consistently are those that integrate documentation and clinical decisions into a single workflow system from the outset. This is not primarily a technology question. It is a design question. You can have the most sophisticated audiology software available and still produce inconsistent outcomes if the underlying process logic is fragmented.
Proactive scheduling is the other area where we see the greatest gap between intention and practice. Most clinics operate on reactive recall, waiting for patients to become overdue before making contact. Graduated reminder touchpoints at 90, 60, and 30 days before key milestones, such as device warranty expiry or annual review dates, produce measurably better patient response rates than a single overdue notice. The message at each touchpoint should carry value, not just a date.
Remote care is genuinely effective when it is decision-guided. The temptation to default everything to remote delivery to reduce costs is understandable, but it creates its own risks. Triage protocols based on clinical flags and patient-reported outcomes are what make remote pathways safe and sustainable. Training your team to apply those triage rules consistently is as important as the technology itself.
— EARS
Supporting your hearing health workflow with professional ear care
A well-functioning hearing care pathway depends on accurate clinical foundations, and that begins with clear ear canals. At Earhealthservice, EARS Clinics provide NHS-accredited earwax removal using microsuction, irrigation, and manual instrumentation, all performed by trained Aural Care Specialists registered with Healthcare Improvement Scotland. Appointments are available in clinic, as same-day bookings, or as home visits across Glasgow and Edinburgh, with costs from £60 for adults. For clinicians looking to develop their own competence, EARS Clinics also offer microsuction training courses aligned with current best practice standards. To refer patients or book directly, visit the full range of earwax removal procedures available at EARS Clinics.
FAQ
What does improving hearing health workflow mean in practice?
Improving hearing health workflow means applying standardised clinical protocols across earwax removal, audiological assessment, hearing aid fitting, and structured follow-up, supported by digital tools and evidence-based scheduling. The goal is consistent patient outcomes and reduced clinical variability across all practitioners and sites.
When should follow-up appointments be scheduled after hearing aid fitting?
NICE 2026 guidance specifies a face-to-face audiology follow-up 6 to 12 weeks after hearing aid fitting, covering comfort, sound settings, cleaning, battery management, and logged usage hours. This timing is now a clinical standard rather than a discretionary scheduling choice.
Is remote hearing care as effective as in-person appointments?
Remote cochlear implant programming is clinically equivalent to in-person programming for stable adult patients, with high satisfaction reported by both patients and clinicians. However, triage protocols are required to identify when in-person escalation is necessary, particularly for paediatric cases or patients reporting sudden changes in hearing.
How does self-directed auditory rehabilitation fit into a clinical workflow?
Self-directed auditory rehabilitation, delivered via computer-based programmes or mobile applications, produces meaningful speech recognition improvements when patients complete 20 or more hours of training. It should be prescribed formally at the hearing aid fitting appointment as part of the care plan, not offered as an optional add-on.
What is the most effective way to reduce clinical variability across a multi-site audiology practice?
Standardising mandatory data capture within audiology software and treating documentation, billing, and clinical decisions as one integrated system is the most effective approach. Embedding guided clinical workflows directly in software enforces consistency without relying on individual practitioner memory or habit.
Recommended